IMPLANT TREATMENT PLANNING
USING A PATIENT ACCEPTANCE PROSTHESIS, RADIOGRAPHIC RECORD BASE, AND SURGICAL TEMPLATE
EDward M. Amet, DDS, MSD
Scott D. Ganz, DMD
The use of a patient acceptance prosthesis as a radiographic record base after incorporation of a radiopaque medium to optimize information from computerized tomography scans for implant planning and prosthodontic design is presented. The patient acceptance prosthesis can also be used as a surgical template. By receiving the patient’s acceptance of the prosthesis before CT scans are done, the potential for success is increased. (Implant Dent 1997;6:193-197)
Successful implant treatment is directly related to achieving integration and restoring hard and soft supporting structures, esthetics, and function.l-5 It is necessary for the clinician to visualize the final prosthetic result before implant placement and to have a thorough understanding of the surgical and prosthodontic phases of treatment to achieve a predictable outcome. 6-12
Advances in computer software technology have enabled digitized information from computerized tomography (CT) scans to be used for implant placement planning. The clinician can view and interact with the CT scan data to presurgically place the implant body and visualize the prosthodontic implications.
The clinical evaluation of the edentulous patient is based on visual examination, manual palpation, gauging tissue thickness, and evaluation of soft tissue quality. An appropriate radiographic assessment and accurate pretreatment mounted diagnostic casts are also necessary. During the diagnostic phase of implant treatment, a treatment prosthesis is fabricated for the proposed surgical site following conventional prosthodontic protocol. Patient acceptance of the prosthesis will aid in determining if a fixed or removable overdenture prosthesis is indicated and if grafting is required to change the type of prosthesis. The esthetic and functional positions of the teeth should be determined and accepted by the patient before any radiographic or surgical intervention using the individualized patient acceptance prosthesis (Fig.1).13 After evaluation and patient approval, the acceptance prosthesis or a duplicate of the existing prosthesis can be used as a CT scan record base (Fig. 2).
The most frequently used radiograph to survey implant sites is the panoramic view. A panoramic radiograph provides a two-dimensional picture and reveals little of the true, often complex, three-dimensional bony anatomy. It is not uncommon to discover anatomic conditions different from those anticipated based on the limited available information. When implant placement is considered in close proximity to vital structures, a computerized tomographic survey (CT scan) is required for diagnostic and surgical accuracy.14 The CT scan produces a distortion-free, three-dimensional image of the underlying bone that can be further enhanced by the use of a radiopaque CT scan record base.


CT scans generate volume images from digitized information, resulting in three views of the bony anatomy (axial, panoramic, and cross-sectional oblique). Accurate measurements can be made directly from the CT scan film, because of a 1 to 1 reproduction. Each image visualizes anatomic sections in 1mm increments, resulting in precise documentation of the bony configuration. The three-dimensional images show bone height, length and width of the proposed implant site. Critical anatomic structures (i.e., inferior alveolar canal, maxillary sinus, nasal cavity, mental foramen) can be precisely located. The residual alveolar ridge, the trajectory and angulation of the proposed implants, the submandibular fossa, and any unsuspecting irregularities in ridge structure can be visualized, eliminating potential surgical and restorative complications.
Software technology advances (SIM/PlantTM; Columbia Scientific Incorporated, Columbia, MD) allow the CT scan digital information to be used on desktop or notebook personal computers.15 The three radiographic views can be viewed simultaneously and individually magnified, allowing the clinician to view and interact with the CT scan data on the computer monitor (Fig. 3). It is also possible to presurgically represent the proposed implants, grafting sites, and prosthetic abutments, avoiding potential restorative problems (Figs. 4 and 5).
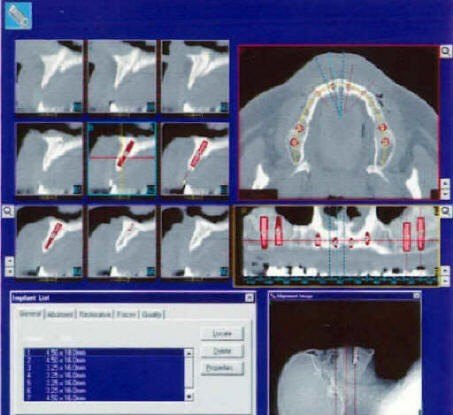

Fig. 3. A three-dimensional view of a SIM/Plant case showing A, presurgical implant placement in the maxilla and a magnified view of radiopaque composite resin in the acceptance prosthesis(B).The CT scan can create a computer-aided design/stereolithography application (CAD/SLA) model on which a subperiosteal or ramus frame implant can be designed and constructed using the analog of the mandible.l6 The CAD/SLA model can also be used for diagnostic mounting and endosteal implant placement planning.
The CT scan record base facilitates identification of implant-crown and implant-connecting bar trajectory, implant position, the occlusal plane, and alveolar ridge. The record base must represent the definitive prosthesis form to optimize assessment of required grafting and implant location relative to the patient’s esthetic and functional requirements. The patient’s original prosthesis, acceptance prosthesis, or a duplicate of the acceptance prosthesis can be used as a CT scan record base and surgical template. Postoperatively, the patient’s original prosthesis or the acceptance prosthesis is used during the healing phase.
A number of techniques for the construction of CT scan record bases have been described in the literature. 17-19PATIENT REPORT
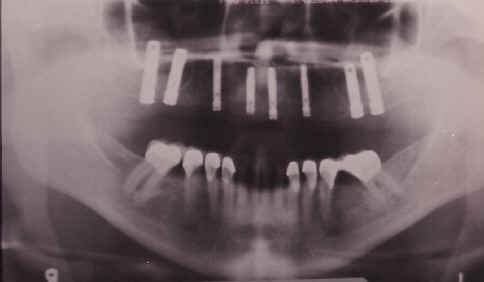
A 42-year-old African-American woman who had been using a maxillary complete denture since 1977 requested a fixed prosthesis. A preoperative panoramic radiograph revealed insufficient posterior bone for posterior implant placement. A bilateral maxillary sinus elevation with subantral augmentation was completed and allowed to heal for 4 months. A patient acceptance prosthesis was subsequently fabricated (Fig. 1) which also served as a CT scan record base after placement of a radiopaque composite resin in reference sites (Fig. 2). A duplicate of the prosthesis was used as a surgical guide during the placement of 8 implants in the maxilla (Fig. 6).
A 54-year-old Caucasian woman presented after 21 years of functioning with complete dentures. A panoramic radiograph revealed the loss of maxillary bone and adequate mandibular vertical bone height (Fig. 7). A tentative treatment plan was developed consisting of a mandibular implant-supported overdenture and a maxillary complete denture. A presurgical CT scan using a radiopaque record base was taken. The scan data was prepared for use with SIM/Plant software, which confirmed the presence of adequate mandibular bone in the symphysis region. Cross-sectional oblique radiographs of the area revealed excellent bone density and width (Fig. 8).
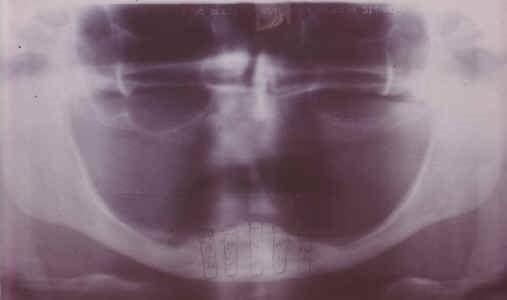
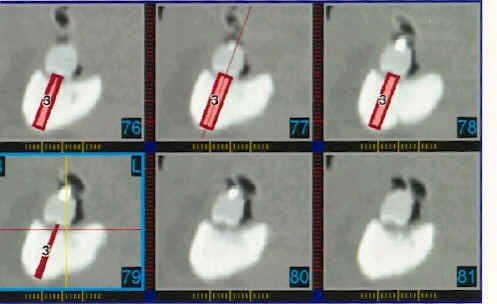
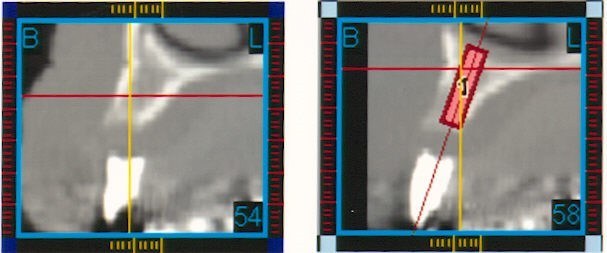
Fig. 8. Cross-sectional oblique radiographs with presurgical SIM/Plant planning and placement for implants in mandible.On the day of surgery, the CT scan record base was modified for use as a surgical template and five threaded implants were placed in the mandibular symphysis region with the angulation selected to increase the A-P spread and obtain bicortical stabilization. The cortical crest was grafted with resorbable hydroxyapatite to facilitate recontouring of the buccolingual concavity. The premaxilla was grafted with dense hydroxyapatite to obtain optimal ridge contour. Figure 9 shows the implants in place in the mandible.
CONCLUSION
The use of an acceptance prosthesis and a radiographic record base during CT imaging enhances pretreatment implant positioning, grafting requirements, and final prosthesis design. Idealized implant location and grafting requirements are subsequently transferred to the surgical template, thereby facilitating the definitive prosthodontic treatment. Patient approval of the acceptance prosthesis before the CT scan will increase the potential for success. The acceptance prosthesis can be used as a radiographic record base and a surgical template.
Contact Reconstructive and Implant Dental Center at 913-534-8801 to learn how our experienced prosthodontist is determining ideal implant position with computed tomography in Overland Park, Kansas. We can answer any question you have when you visit with Dr. EDward M. Amet.
REFERENCES
1. Engelman MJ, Sorensen JA, Moy P. Optimum placement of osseointegrated implants. J Prosthet Dent 1988;59:467-473.
2. Reike DF. Esthetic and functional considerations for implant restoration of the partially edentulous patient. J Prosthet Dent 1993;70:433-7.
3. Murell GA, Davis WH. Presurgical prosthodontics. J Prosthet Dent 1988;59:447-452.
4. Smith DE, Zarb GA. Criteria for success of osseointegrated endosseous implants. J Prosthet Dent 1989;62:567-572.
5. Ganz, S.D., What is the most important aspect of implant dentistry? Implant Soc. 1994;5:2-4
6. Daftary, F, Bahat O., Prosthetically formulated natural aesthetics in implant prostheses. Pract Periodont Aesthetic Dent 1994;6:,75-83.
7. Langer B. Solutions for special bone situations. Int J Oral Maxillofac Implants. 1994;9:(suppl):21.
8. Saadoun AP, Sullivan DY, Krichek M, et al. Single tooth implant: management for success. Pract Periodont Aesthet Dent 1994;6:73-82.
9. Parel SM, Sullivan DY. Esthetics and Osseointegration. Dallas, Taylor Publishing Company; 1989:19-112.
10. Mecall RA, Rosenfeld AL. The influence of residual ridge resorption patterns on implant fixture placement and tooth position. Part 1. Int J. Periodont Rest Dent.1991;11:9-23.
11. Lazzara, RJ. Criteria for implant selection: surgical and prosthetic considerations. Pract Periodont Aesthetic Dent. 1994;6:55-62.
12. Saadoun AP, LeGall, M. Implant positioning for periodontal, functional, and aesthetic results. Pract Periodont Aesthetic Dent 1992;4:43-54.
13. Amet EM. Fixed provisional restorations for extended implant treatment: Part I J Oral Implantol. 1995; 21: 201-206.
14. Schwarz MS, Rothman, SLG, Chafetz N., et al: Computed tomography in dental implantation surgery. Dent Clin North Am 1989;33:555-597.
15. Sethi A. Precise site location for implants using CT scans: a technical note. Int J. Oral Maxillofac Implants 1993;8:433-438.
16. James RA, Lozada JL, Truitt HP: Computer tomography (CT) applications in implant dentistry. J Oral Implantol. 1991;17:10-15,
17. Stellino G. Morgano S.M. Imbelloni A. A dual-purpose, implant stent made from a provisional fixed partial denture J. Prosthet Dent 1995;74:212-214.
18. Ganz, SD., “Interactive cmputer utilization for treatment planning dental implants and optimizing patient communications.” Presented at the AAOMS Conference on Esthetic Implant Rehabilitation in the Partially Edentulous Patient ; October 20, 1995;Chicago, IL.
19. Ganz, SD. The use of computer imaging technology. Presented at the joint meeting of the Academy of Osseointegration and the European Association of Osseointegration on Implant Rehabilitation of the Compromised Patient; October 20, 1996; Amsterdam, The Netherlands.
CAPTIONS
Fig. 1. The patient acceptance prosthesis in occlusion with a mandibular stone cast.
Fig. 2. The CT scan record base can be used for accurate implant site location.
Fig. 3. A three-dimensional view of a SIM/Plant case showing A, presurgical implant placement in the maxilla and a magnified view of radiopaque composite resin in the acceptance prosthesis(B).
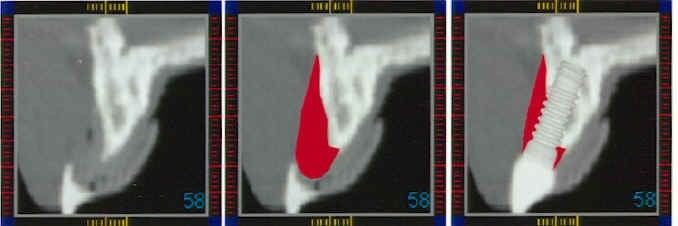
Fig. 4. The radiopaque tooth incorporated into a preoperative CT scan showing the relationship of the existing bone(A), proposed graft(B), and proposed implant reconstruction(C).
Fig. 5. A, Full contour radiopaque tooth on the CT scan image. B, Projected implant location relative to the clinical position of the denture tooth.
Fig. 6. Postoperative panoramic radiograph showing implants in place in the maxilla.
Fig. 7. Preoperative panoramic radiograph of edentulous mandible with outlines of implants sketched in symphysis region.
Fig. 8. Cross-sectional oblique radiographs with presurgical SIM/Plant planning and placement for implants in mandible.
Fig. 9. Postoperative panoramic radiograph with implants placed in mandible.
IMPLANT TREATMENT PLANNING USING A PATIENT
ACCEPTANCE PROSTHESIS, RADIOGRAPHIC RECORD BASE,
AND SURGICAL TEMPLATE. PART 1: PRESURGICAL PHASE
Reprint requests to:
Dr. EDward M. Amet
10801 West 87th Street, Suite 100
Overland Park, KS 66214