Beauty is obvious to the observer but is difficult to quantify. Many believe that our concepts of beauty originated with the Egyptians and from Greco-Roman tradition. The image of queen Nefertiti (@ 1350BC) remains influential even in these modern times. The Egyptian aesthetic ideal included a broad face, aquiline nose, prominent eyes, full lips, and a relatively prominent chin. Our historic concept of beauty and our “standards” for facial proportions also derive from Greco-Roman tradition. During the Renaissance, masters such as Leonardo da Vinci undertook artistic and mathematical facial analysis that influence our ideas about beauty to this very day.

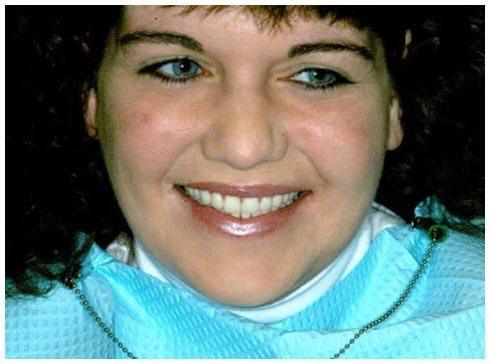
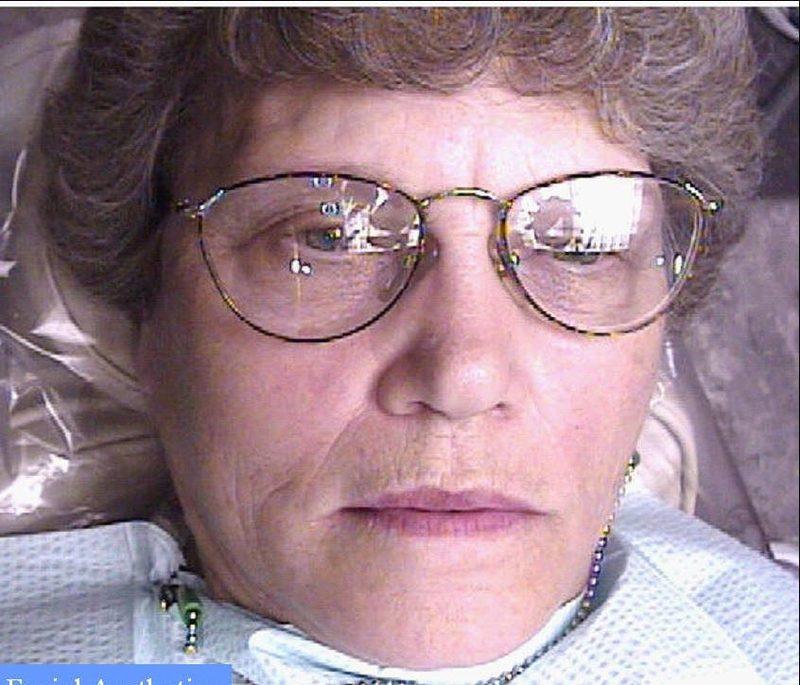
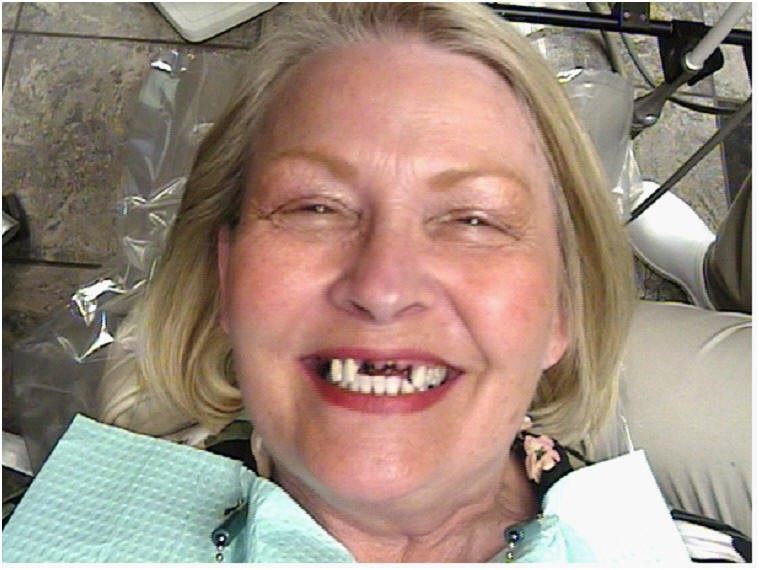
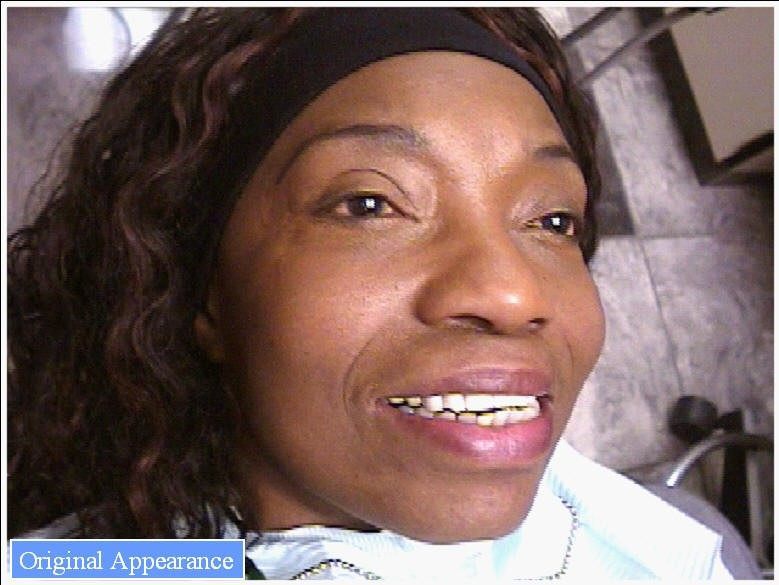
The dentist treating a patient with missing or damaged teeth can do much to improve the beauty and natural appearance of the facial. The appearance of the entire lower half of the face depends on the teeth and their supporting structures. It is usually not difficult on casual meeting to detect a person who is has dental aesthetic needs. The characteristic thin drooping upper lip that appears lengthened and has a reduced red vermilion border is typical of malposition anterior teeth as well as a reduced Occlusal Vertical Dimension (OVD) as measured between the chin and nose.

Tense wrinkled lips often reveal the person’s effort to hold their dentures in place or the inability to naturally show their existing teeth. The prosthetic teeth may have been positioned too high from the vermilion border of the upper lip and back too far from the lip for proper support. The selected teeth may have too low a value or appear too dark especially if they have been positioned too far back in the mouth. The drooping corners of the mouth tell the story of the misshapen and misplaced dental arch form of the anterior teeth, the thin denture borders, and often reduced OVD.


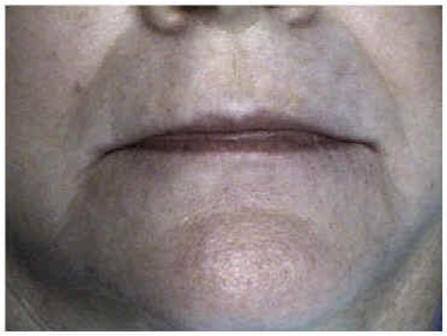
The result is the appearance of premature aging which is caused not by age itself but by the lack of support for the lips and cheeks due to the loss or improper placement of teeth. The apparent extra fullness of the lower lip may be the result of too broad a lower dental arch or the elimination of the natural groove below the lower lip, the mentolabial sulcus. This may indicate that the lower anterior teeth have been placed too far toward the tongue or that the lower denture flange is over extended or too thick.


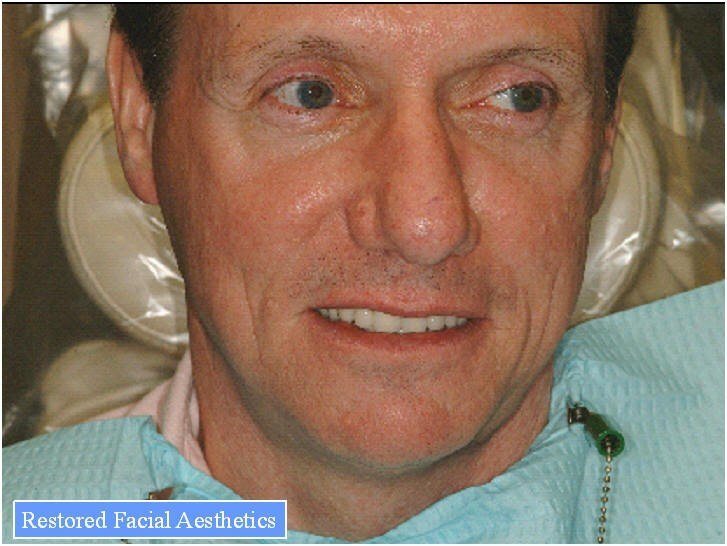
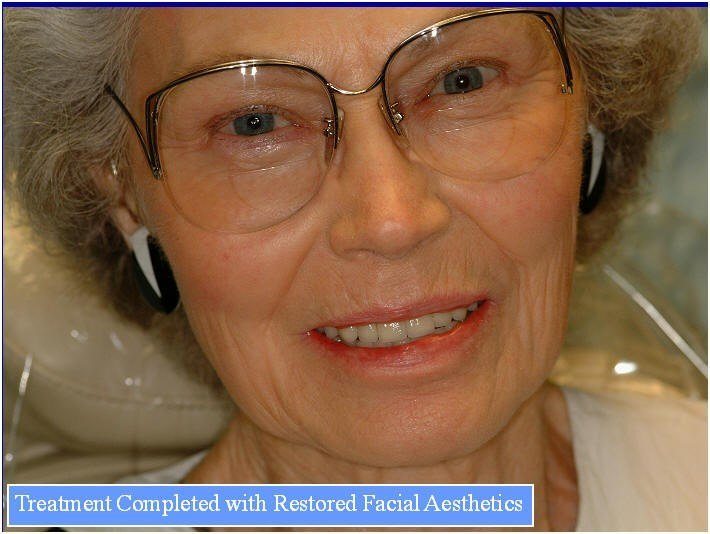
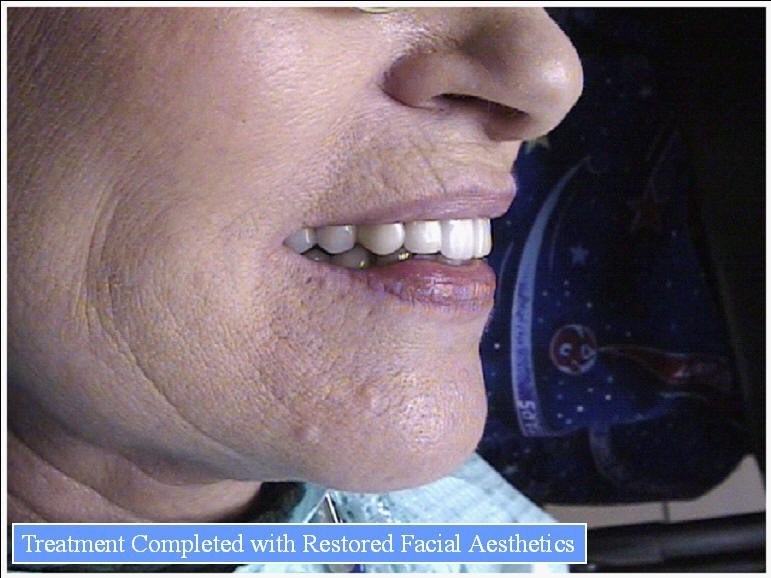
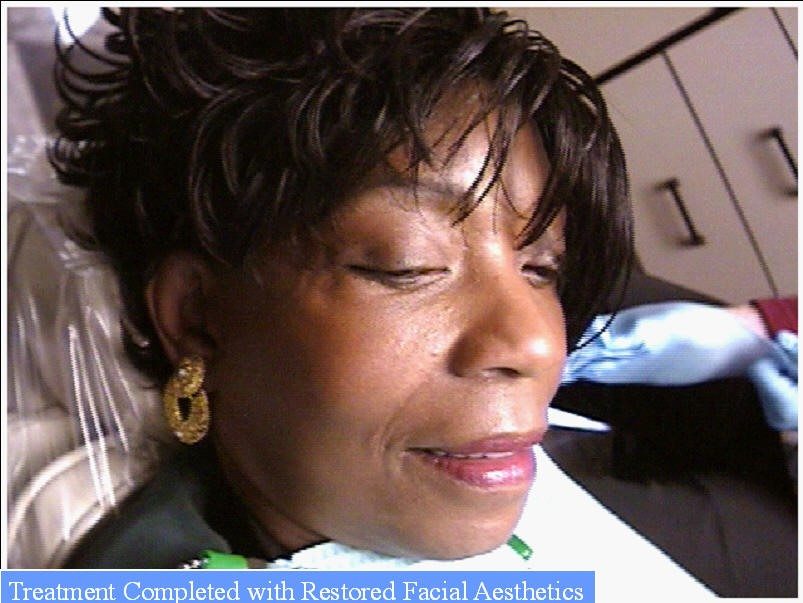
RESTORING FACIAL AESTHETICS
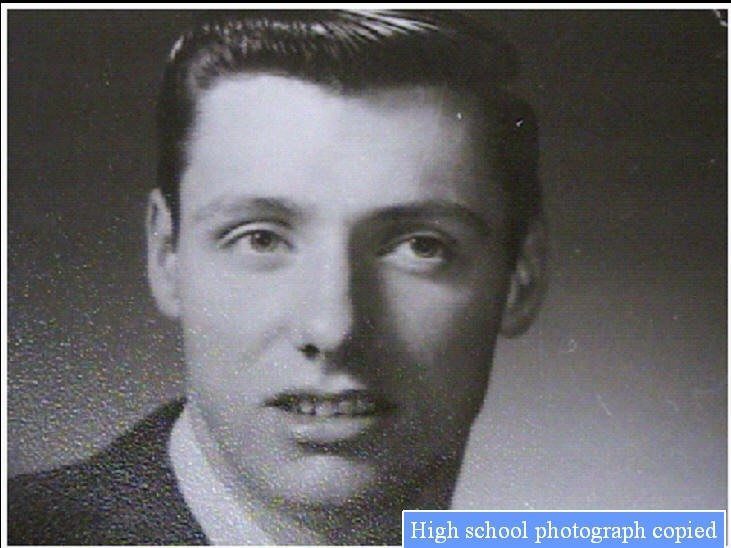
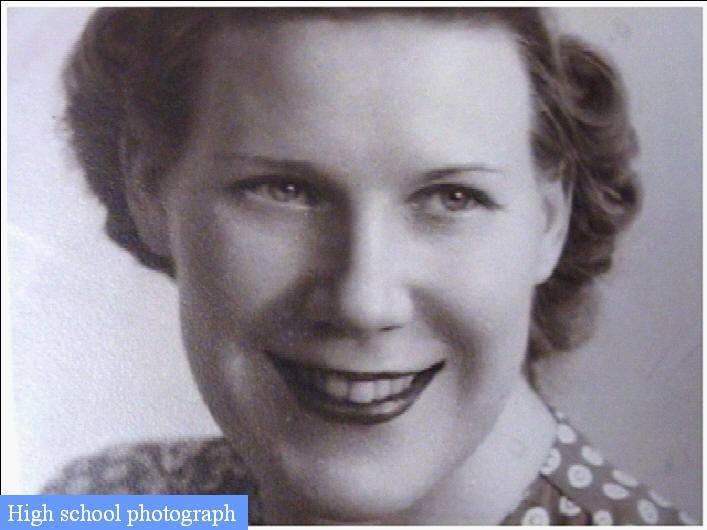
Studying the dental and facial appearance and landmarks of a patient at a younger age from photographs before attempting to achieve the goal of restoring facial aesthetics will often result in a better result.
The facial landmarks of the lower third of the face have a direct relationship to the presence of the natural teeth. The contours of the lips depend on their intrinsic structure and the support for them provided by the teeth or the denture bases behind them.
When the natural teeth are lost, these landmarks and surrounding facial tissues become distorted. To reestablish normal appearance and function, prosthetic teeth must be replaced in the same position as the natural teeth that were lost.
The lips vary in length, thickness, shape, and mobility in different patients. Such variance accounts for the degree of visibility of the upper and lower anterior teeth during speech and other facial expressions.

When the mandible is in the resting position the lips usually contact each other and turn slightly outward, exposing the vermilion border. The philtrum is the vertical groove in the upper lip and the horizontal depression midway between the lower vermilion border and the chin is the mentolabial sulcus.
Incorrect positioning of the anterior teeth or supporting base of the prosthesis will alter the normal appearance of the vermilion border, the philtrum, and the mentolabial sulcus in the patients.
The nasiolabial sulcus or groove, is a depression in the skin on each side of the face which runs angularly outward from the ala of the nose to the corners of the mouth. The zygomaticus originates on the zygomatic bone and angles downward to insert at the corners of the mouth into the orbicularis oris.

The action of the two zygomatici in elevating the corners of the mouth for smiling produces the nasolabial sulcus. Many older patients want to have the nasiolabial sulcus obliterated because it becomes a wrinkle as the skin loses resilience.

The sulcus is normal and should not be eliminated. The proper treatment is to bring the entire upper dental arch forward to its original position when the teeth were present and to maintain the original arch form of the natural teeth and supporting structures.
In many patients the upper lip rests on the labial surfaces of the upper anterior teeth, and the lower lip on the labial surfaces of the lower anterior teeth and incisal edges of the upper teeth. For this reason, the edge of the lower lip should extend outward and upward from the mentolabial sulcus.

A study of the inclination of the osseous structure supporting the lower anterior teeth indicates that, in most patients, the clinical crowns of the lower teeth are labial to the bone that supports them and the upper lip functions on an incline.

Neglect of these factors in the replacement of natural teeth will often cause the lip to be ill formed and in time lead to the formation of vertical lines in the lip.

After an acceptable OVD has been determined and the horizontal relation of the casts on the articulator has been verified for centric relation, the appearance of the patient is studied and then modifications are made in the arrangement of the teeth to obtain a harmonious effect with the patient’s face.




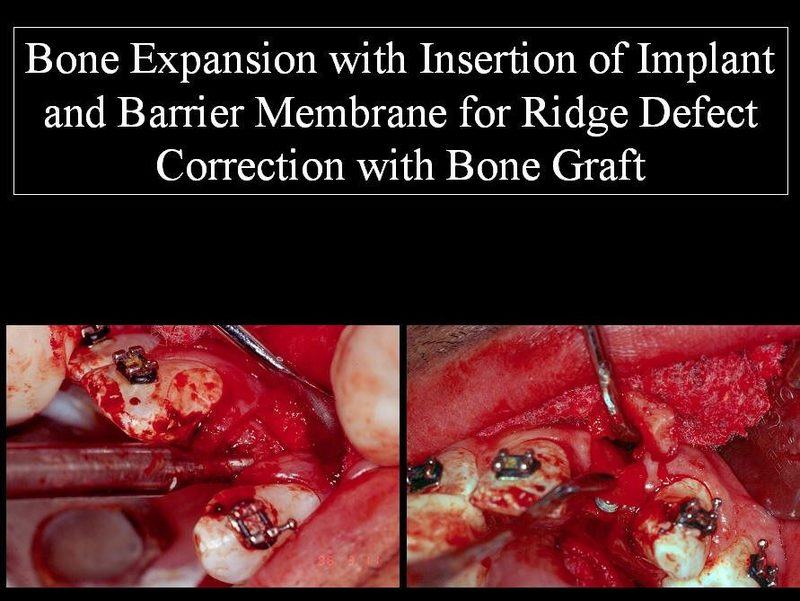
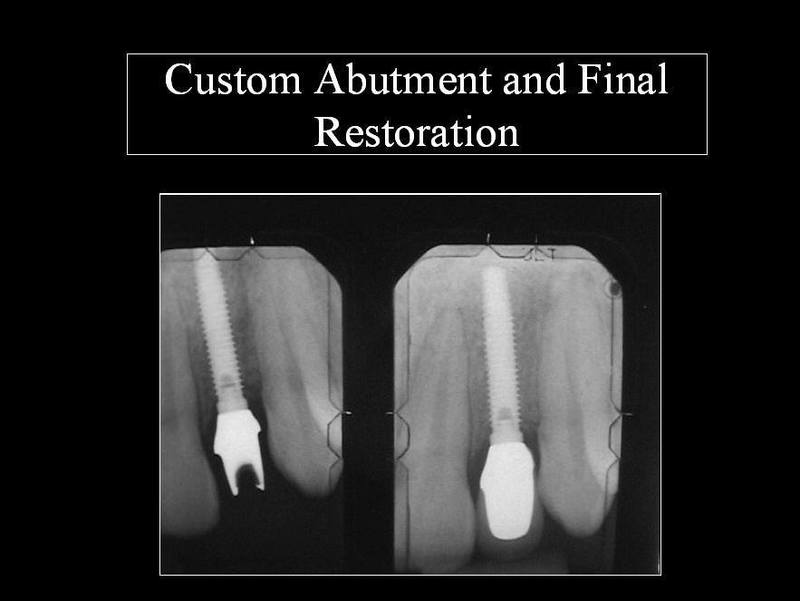
Single Anterior Implant
These restorations present their own challenges to the dentist, not only in placement and bone expansion or bone grafting, but in the final restoration to achieve realism.

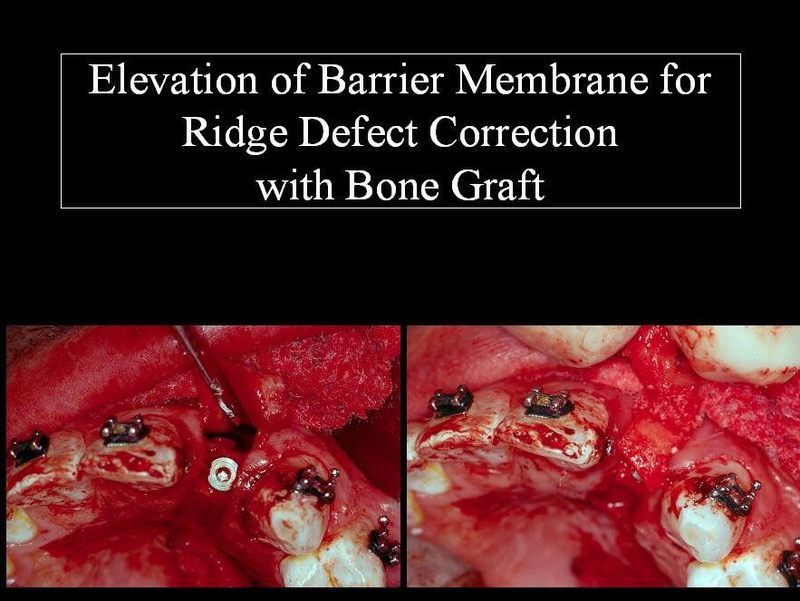
The soft tissue needs to surround and frame the final restoration creating the natural contours present around adjacent natural teeth. Ridge deformities need to be corrected to achieve this.

On casual meeting, it is usually not difficult to detect a person who has artificially constructed crowns as a dark line at the gum tissue or bulky thick teeth detracts from any realism.

The more sophisticated PFM crowns use a multi-layering porcelain technique and the color is built within and may have eight or more porcelain layers. Finally, the artistic skill of the dentist and technician determines the end result.

The success of dental implants in the treatment of patients is directly related to good treatment planning. The goal of implant dentistry is to achieve integration of implants and restorative treatment which replaces a missing tooth or teeth and lost supporting structures, as well as to restore proper aesthetics and function.

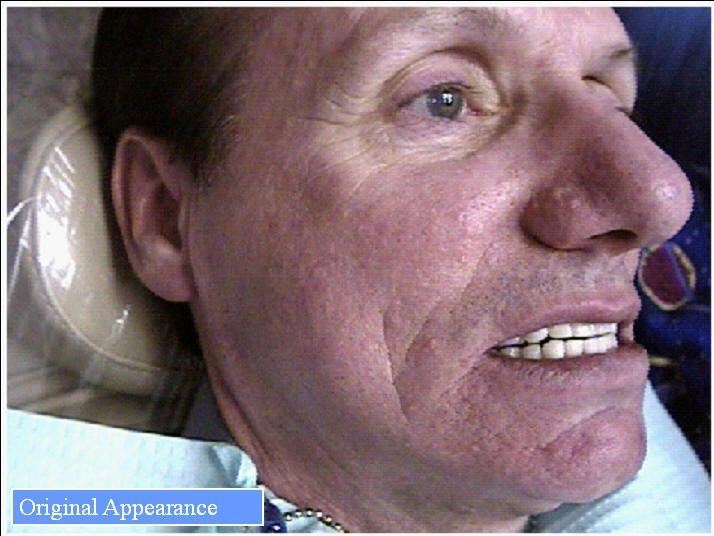
Original Appearance
To achieve this goal, it is necessary for the dentist and patient to be able to visualize the final prosthetic results prior to surgical implant placement. Therefore, it is essential for the dentist to have a thorough understanding of both phases of treatment in order to diagnose, treat and restore natural appearance.

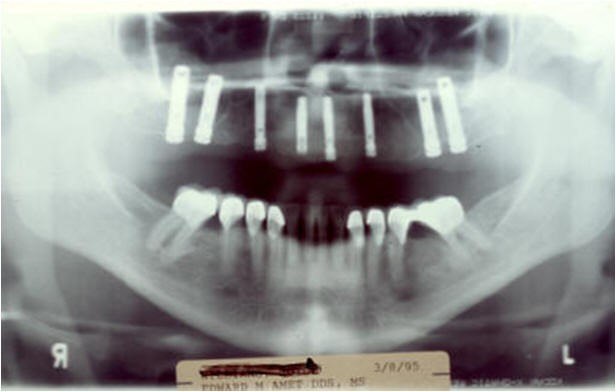
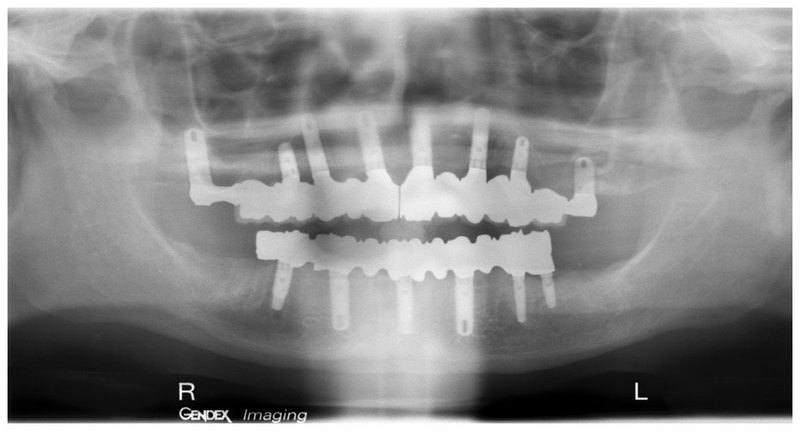
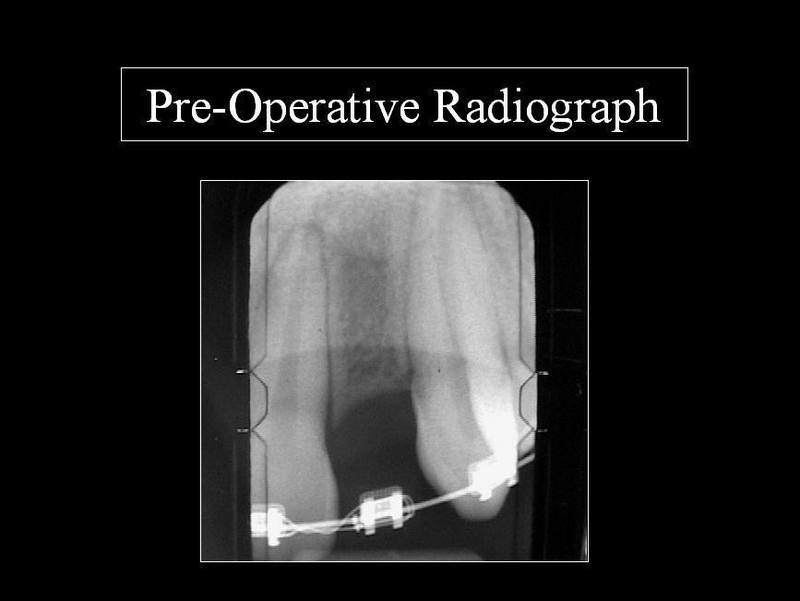
Initial Radiograph
The clinical evaluation of the totally edentulous patient is based on an implant examination with evaluation of soft tissue quality.

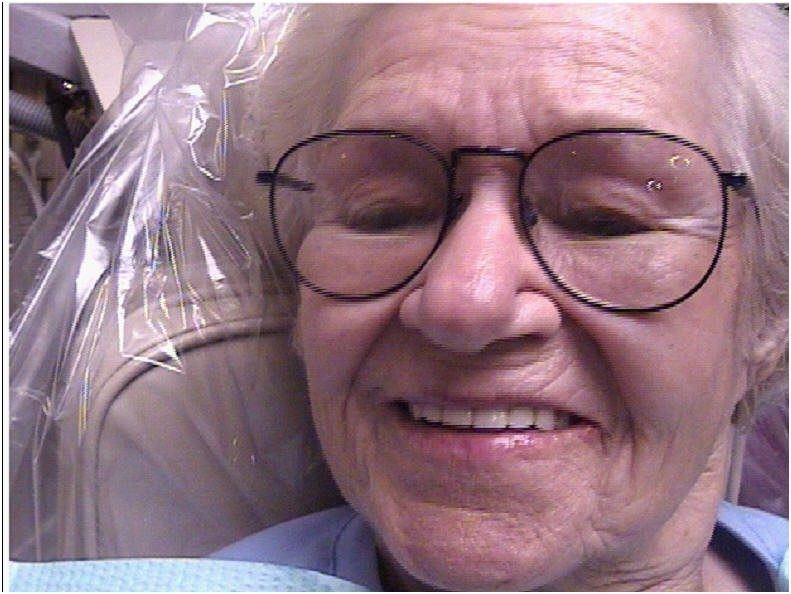
Original Appearance
Appropriate X-rays are needed, as are accurate pre-treatment mounted diagnostic casts. Likewise, during the diagnostic phase of implant treatment planning, a conventional prosthodontic protocol is followed.

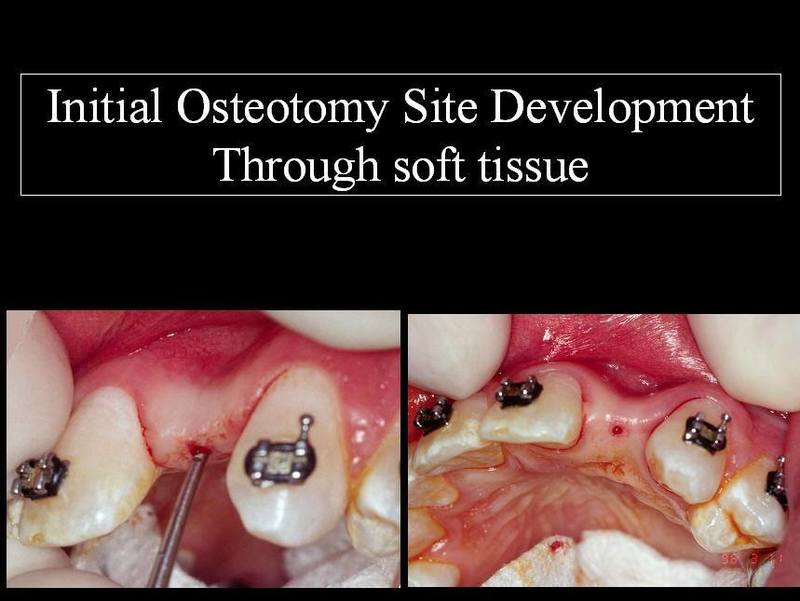
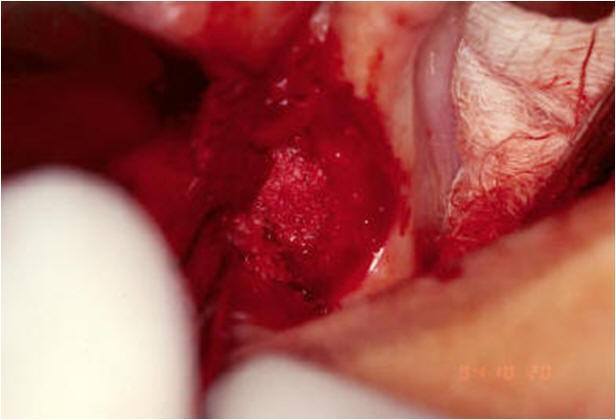
Start of Sinus Surgery
This facilitates the construction of treatment teeth for the proposed surgical sites. Patient acceptance of these teeth or prosthesis will aid in determining if a fixed bridge or overdenture prosthesis is indicated or if grafting is required to change the type of prosthesis.

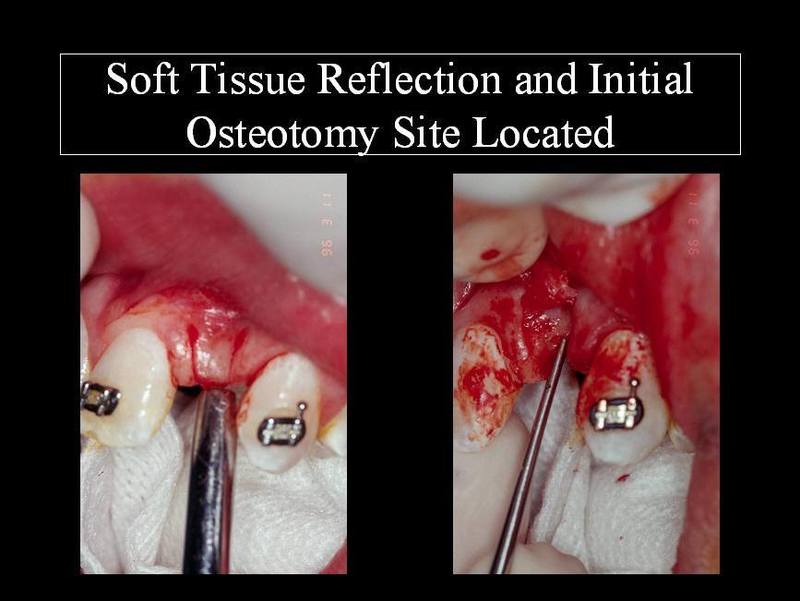
Lateral Entrance Into Maxillary Sinus With “Collatape”
The aesthetic and functional position of the teeth should be determined and accepted by the patient prior to any X-rays or surgical intervention using this prosthesis. Once evaluated and approved by the patient, a duplicate is constructed for radiographic implant determination.
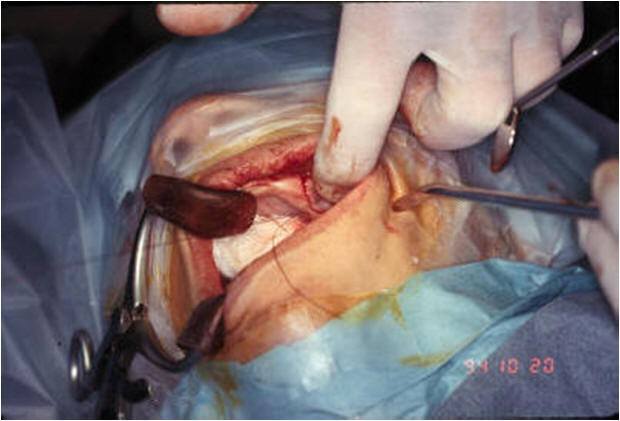
Grafting Into Sinus Cavity
The most frequent X-ray utilized to survey implant sites is the dental panoramic view. This provides a two-dimensional view and reveals little of the true, often complex, three-dimensional bony anatomy.
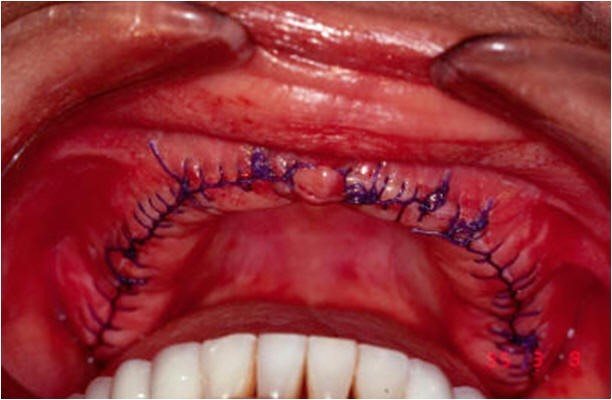
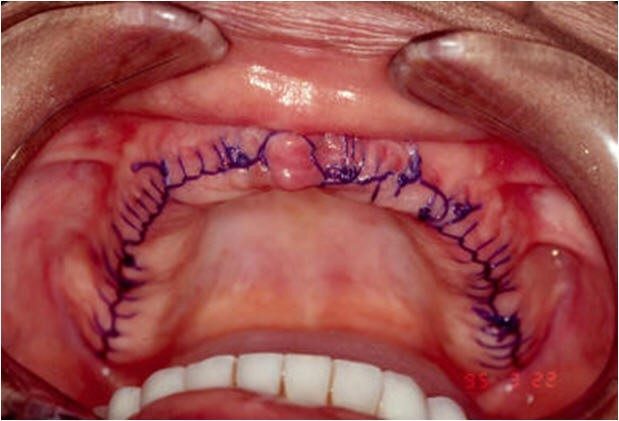
Suture Closure of Opening Into Sinus
It is not uncommon to discover anatomical conditions different from those anticipated based on the limited information available.
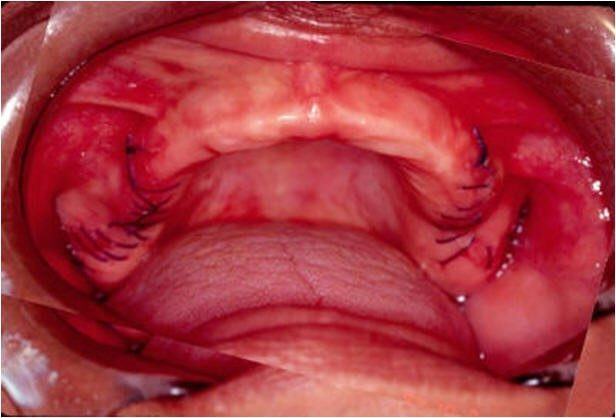
One Day Post-Op From Surgery
When implant placement is considered in close proximity to vital structures a computerized tomographic survey (CT scan) is required for diagnostic and surgical accuracy.
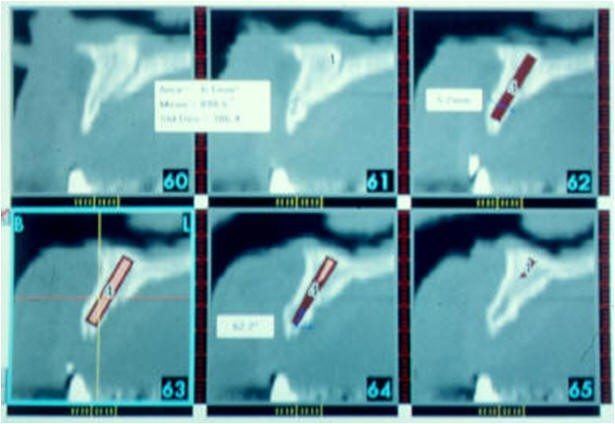
Pre-Op Planning for Implant Placement
The CT scan delivers a distortion-free, three-dimensional image of the underlying bone that can be further enhanced by a radiopaque patient acceptance prosthesis or CT scan record base.
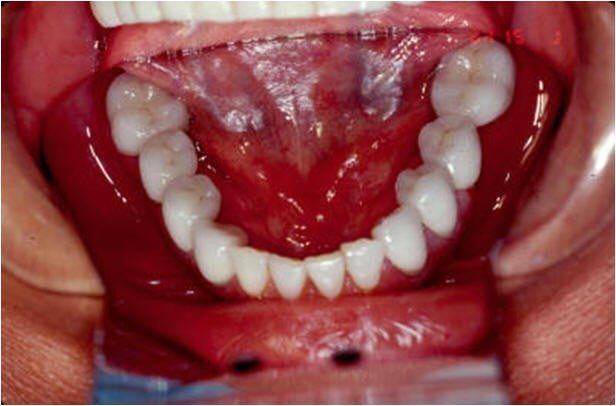
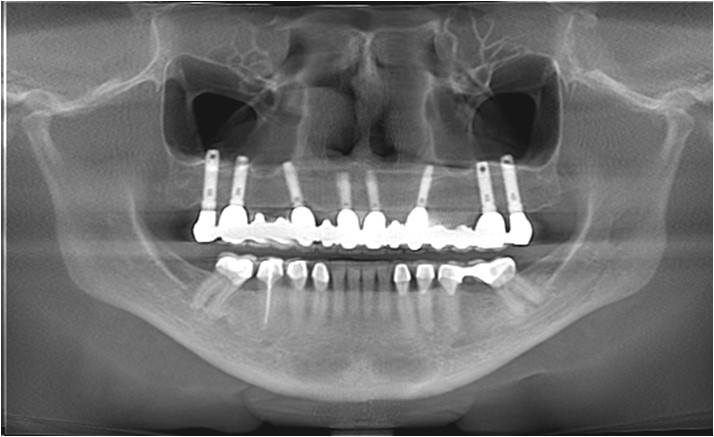
Completed Restorative Treatment of Mandibular Arch
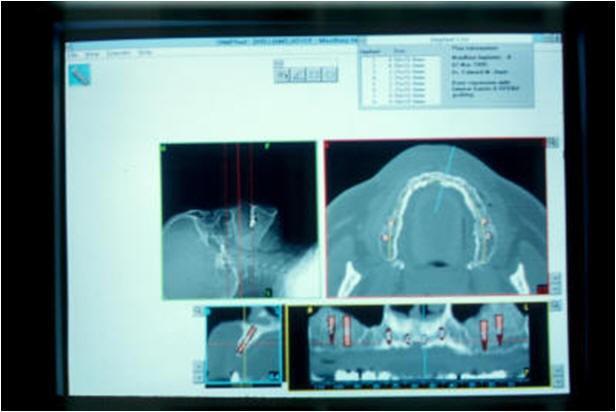
Software technology advances (SIM/Plant,TM Columbia Scientific, Inc., Columbia, MD) permit the CT Scan digital information to be able to be used on desktop or notebook personal computer (PC).

Planning for Aesthetics of the Maxillary RPD
All three radiographic views can be viewed simultaneously, or individually magnified and permit the clinician to view and interact with the CT scan data on the computer monitor. It is also pre-surgically possible to represent the proposed implants, grafting sites, and prosthetic abutments that are there by avoiding potential prosthetic problems.

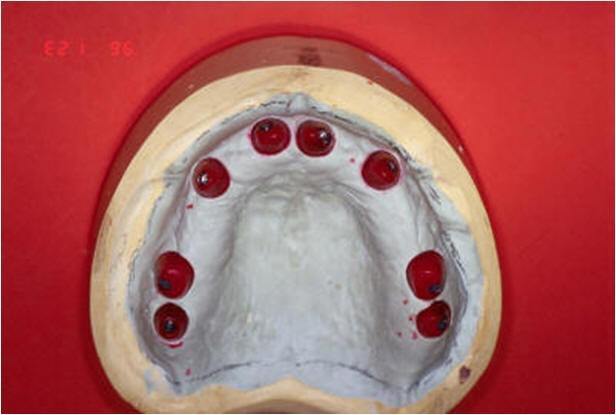
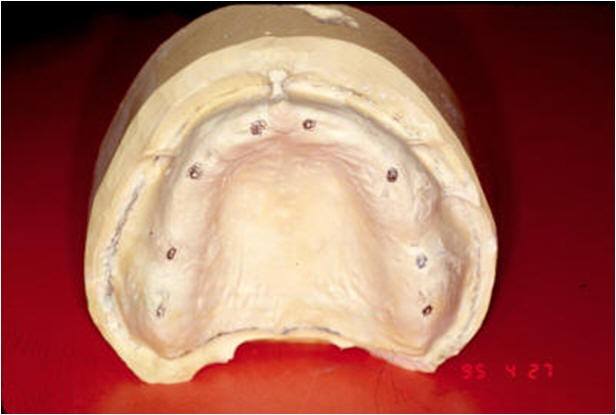
Treatment Denture and Surgical Template for Implant Guide “Patient Acceptance Prosthesis”
The patient acceptance prosthesis is modified with radiopaque markers to make a CT scan record base and utilization in conjunction with the CT scan and facilitate the determination of the prosthetic treatment plan. The prosthetic considerations will dictate the final implant position if grafting or ridge augmentation is needed.