“Classic”
1. All teeth missing.
2. Advanced bone loss mandible.
3. Long-term use of complete dentures.
4. OVD less than ideal, needed to change.
5. Facial aesthetics needed improvement.
2. Advanced bone loss mandible.
3. Long-term use of complete dentures.
4. OVD less than ideal, needed to change.
5. Facial aesthetics needed improvement.
TREATMENT GOALS: RECONSTRUCTION OF THE SEVERELY ATROPHIED MANDIBLE
• Single-stage surgical approach for implant placement with grafting and immediate implant-loading with transitional prosthesis.
• Bone strengthening utilizing banked cancellous bone from human cadaver vertebra and Minimal Invasive Surgical technique.
• Patient always has prosthesis during healing for function and aesthetics.
• Single-stage surgical approach for implant placement with grafting and immediate implant-loading with transitional prosthesis.
• Bone strengthening utilizing banked cancellous bone from human cadaver vertebra and Minimal Invasive Surgical technique.
• Patient always has prosthesis during healing for function and aesthetics.

Pre-Operative Photograph

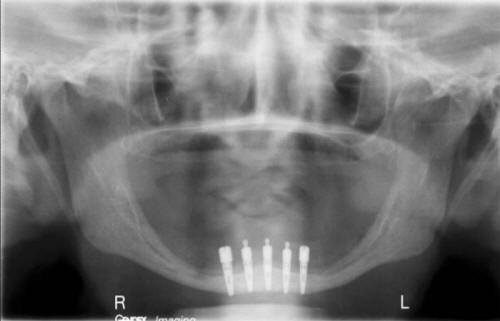
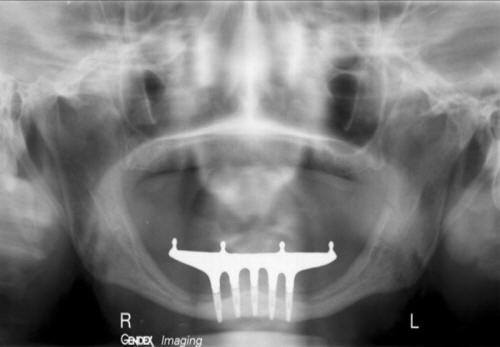
Pre-Operative Radiograph
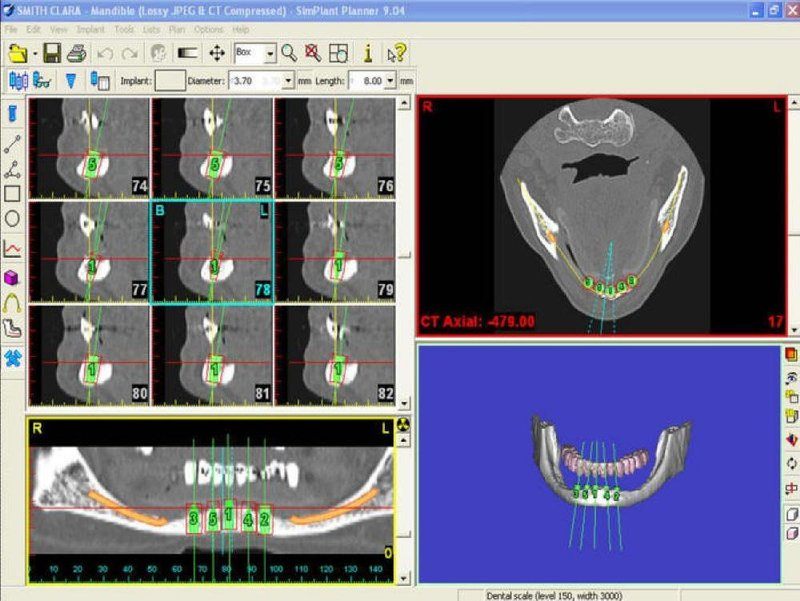
Pre-Op CT Scan Overview Study
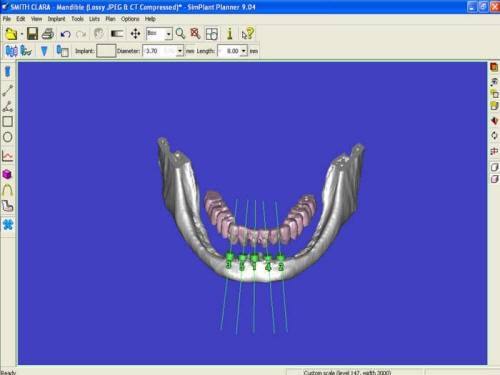
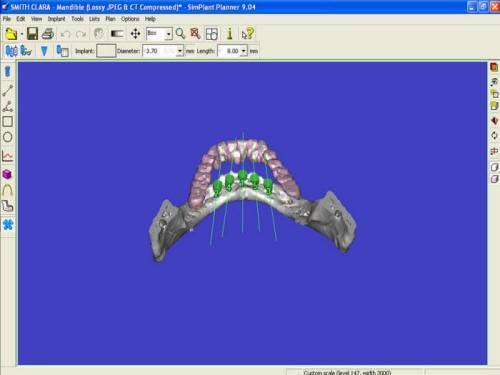
Pre-Op 3D Moveable Translucent Image Showing Advanced Bone Atrophy
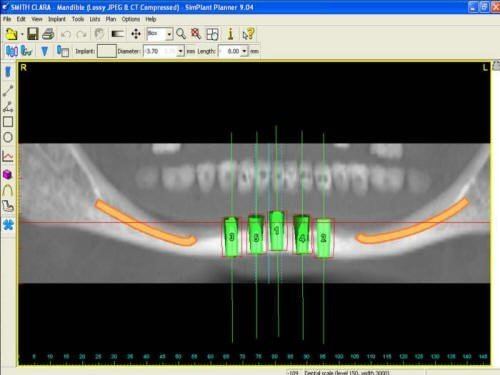
Pre-Op CT Scan Panoramic View
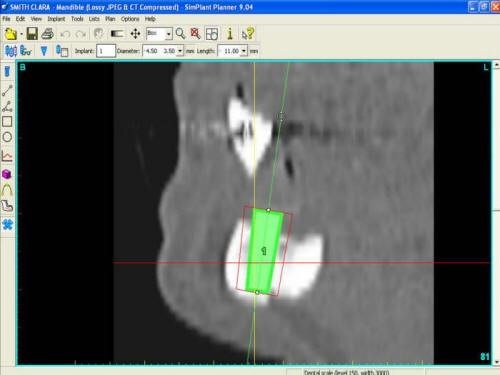
Pre-Op CT Scan Cross Sectional View
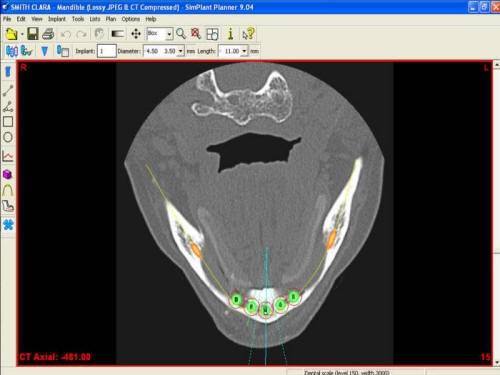
Pre-Op CT Scan Axial View
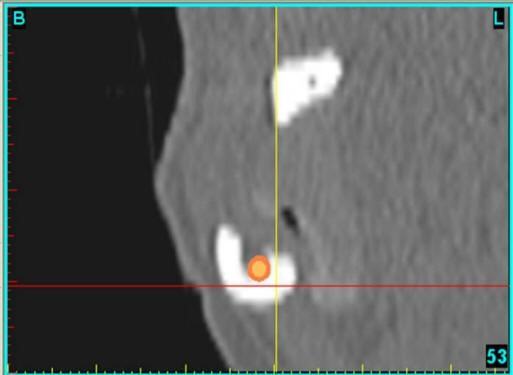
Pre-Op CTS Cross Sectional View Showing Advanced Bone Atrophy Start First Year 4.8mm Mandible

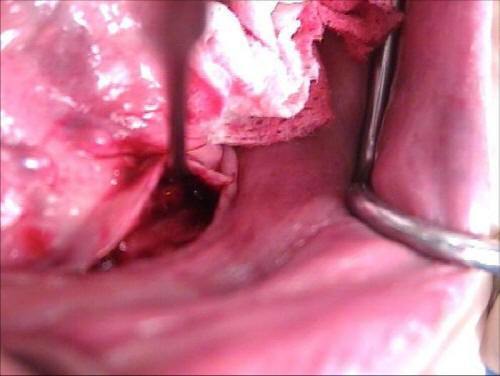
Lingual Tunneling Technique and Creation of Irradiated Cancellous Bone & Marrow Vascularized Site for Bone Graft Placement
TREATMENT GOALS: RECONSTRUCTION OF THE SEVERELY RESORBED MANDIBLE
• Single-stage surgical approach for implant placement with grafting and immediate implant loading with transitional prosthesis.
• Bone strengthening utilizing banked cancellous bone from human cadaver vertebra and Minimal Invasive Surgical technique.
• Patient always has prosthesis (teeth) during healing for function & aesthetics.
• Increase zone of attached keratinized tissue around implants.
• Single-stage surgical approach for implant placement with grafting and immediate implant loading with transitional prosthesis.
• Bone strengthening utilizing banked cancellous bone from human cadaver vertebra and Minimal Invasive Surgical technique.
• Patient always has prosthesis (teeth) during healing for function & aesthetics.
• Increase zone of attached keratinized tissue around implants.

Minimal Residual Keratinized Tissue (Pre-Op)

Increased Residual Keratinized Tissue (Post-Op) 2mm Keratinized Tissue Physiological Increase Keratinized Tissue From 2mm to 5-7mm


1.5mm Minimal Residual Keratinized Tissue Technique for Preservation of Keratinized Tissue Around Implants

1.5mm Keratinized Tissue Divided to Allow Increased Formation of Keratinized Tissue to Surround Implants

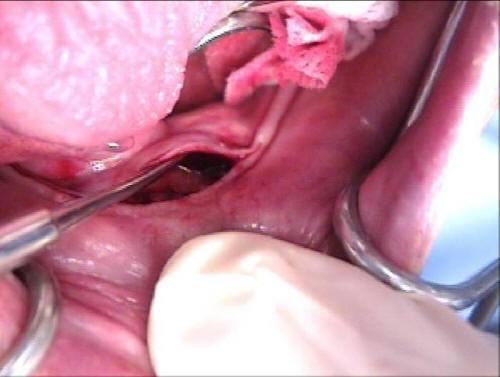
Minimal Tissue Opening to Allow Access and Elevation of Soft Tissue for Creation of Implant sites with Grafting
Lingual Tunneling Technique to Allow Soft Tissue Dissection and Prevention of Inferior Alveolar Nerve Injury
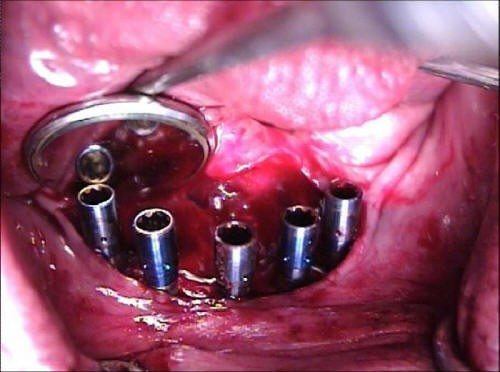
Implants placed prior to Bone Grafting and Healing Screws Placed for Low Height and Access to Grafting Site Then Changed to O-ring Abutments

Lingual Tunneling Technique and Creation of Vascularized Site for Bone Graft Placement
TREATMENT GOALS: RECONSTRUCTION OF THE SEVERELY RESORBED MANDIBLE
• Single-stage surgical approach for implant placement with grafting and immediate implant-loading with transitional prosthesis.
• Bone strengthening utilizing banked cancellous bone from human cadaver vertebra and Minimal Invasive Surgical technique.
• Patient always has prosthesis (teeth) during healing for function & aesthetics.
• Increase zone of attached keratinized tissue around implants.
• Two-week healing with interim prosthesis, then implant connecting bar placed without loading contact of the grafted and healing area with definitive prosthesis.
• Single-stage surgical approach for implant placement with grafting and immediate implant-loading with transitional prosthesis.
• Bone strengthening utilizing banked cancellous bone from human cadaver vertebra and Minimal Invasive Surgical technique.
• Patient always has prosthesis (teeth) during healing for function & aesthetics.
• Increase zone of attached keratinized tissue around implants.
• Two-week healing with interim prosthesis, then implant connecting bar placed without loading contact of the grafted and healing area with definitive prosthesis.

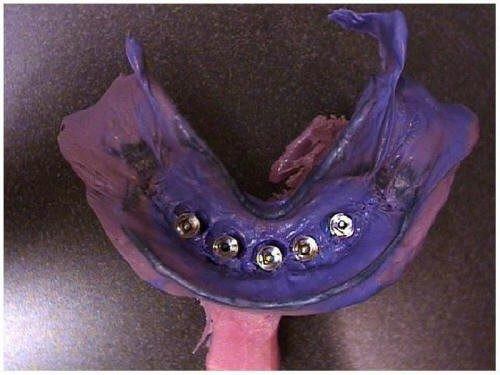
Interproximal Sutures With Attachments Placed Day of Surgery

Interproximal Sutures With O-Ring Attachments Placed Day of Surgery With Rubber Dam in Place Beneath Attachments for Acrylic Pick-Up

Interim Prosthesis With O-Ring Attachments

Pre-made Interim Prosthesis with Picked Up Chair side c Additional Acrylic Resin O-Ring Attachments & Occlusal View Rubber Dam in Place Beneath Attachments

Pre-made Interim Prosthesis With O-Ring Attachments Frontal View

One Day Post-Operative
One Day Implant Placement

Five Days Post-Op Attachments and Immediate Loading
10-14 Days after Surgery M.I.S. Allows for final impression for
implant connecting bar Polyether material of choice for impression
implant connecting bar Polyether material of choice for impression

Three Weeks Post-Operatively

Three Months Post-Operatively
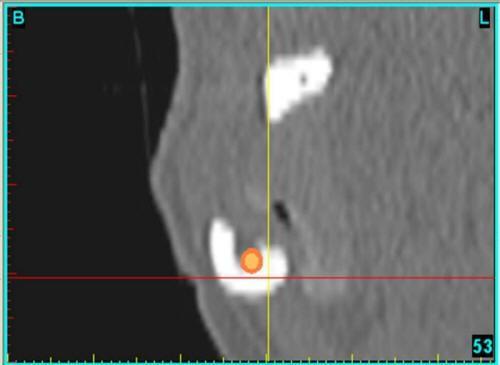
Pre-Op CT Scan Cross Sectional View Start First Year 4.8mm Mandible
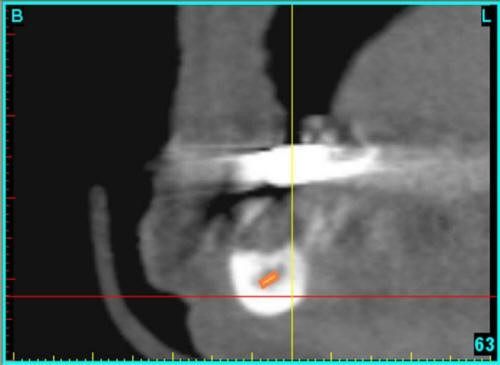
8.75mm Mandible Bone Strengthening Over Nerve Post-Op 1 Year CT Scan Cross Section

Pre-Operative Photograph

Post-Operative Photograph