To learn more about fixed detachable ceramometal reconstruction in Overland Park, Kansas, call 913-534-8801 to schedule with our prosthodontist, Dr. EDward M. Amet, at Reconstructive and Implant Dental Center.
Dental Implant Ceramometal Reconstruction
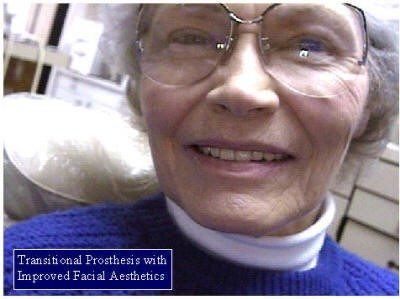
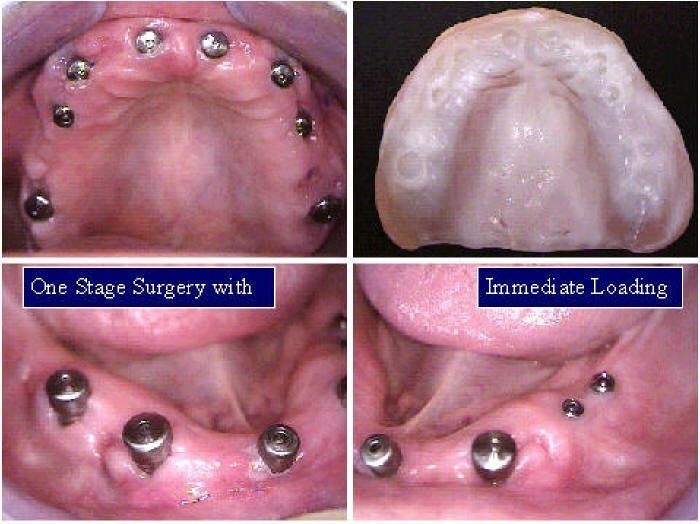
Immediate Extractions With One-Stage Implant Surgery
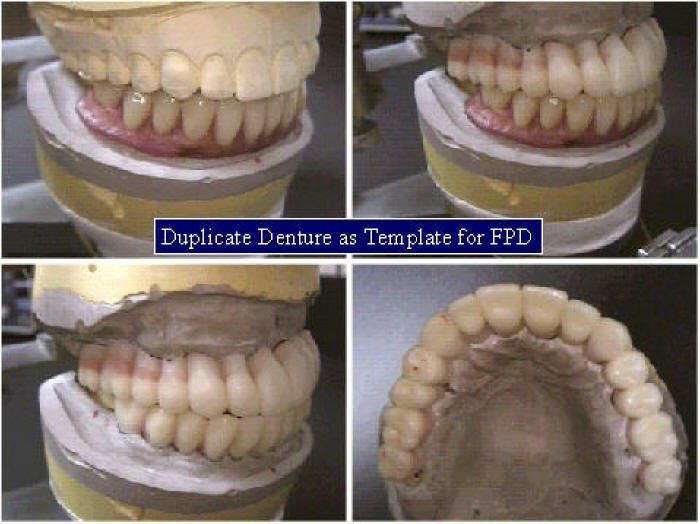
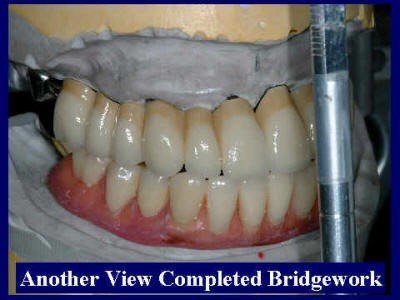
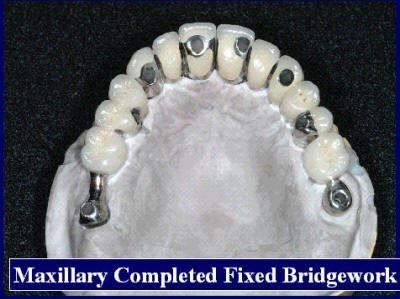
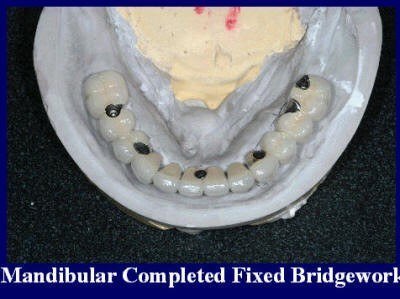
Screw-Retained “Fixed Bridgework”
In preparation for publishing
Treatment Planning and Management From Extractions to Implant Placement and Prosthodontic Reconstruction
EDward M. Amet DDS, MSD, PC
Diplomate American Board of Prosthodontics
Diplomate American Board of Oral Implantology/Implant Dentistry
Joseph P. Milana
Dental Technician
The goal of modern implant dentistry is to return patients to oral health in a predictable fashion. The partially and completely edentulous patient may be unable to recover normal function, aesthetics, comfort or speech with traditional removable prosthesis.
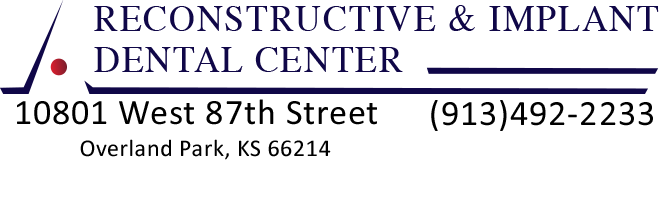
The patient’s chewing and eating ability will often be reduced to 25% of natural dentition when wearing complete dentures. However, an implant stabilized and totally supported prosthesis will often return function to near normal limits. The aesthetics of the edentulous patient are also affected as a result of bone atrophy. Continued resorption leads to irreversible facial changes, with the chin becoming much more prominent and the red border of the lips becoming less visible. The face takes on the appearance of premature aging, with the decreased facial height, which can be corrected with newly designed prosthesis. Correct positioning of teeth will also improve speech especially the silibant or “S” sounds and fricative or “F” sounds, which may have change with the defective prosthesis.
An implant stimulates the bone and maintains its dimension and density in a manner similar to healthy natural teeth. As a result, the patient’s facial features are not compromised by lack of support. In addition, implant-supported restorations are positioned in relation to aesthetics, function, and speech, not in “neutral zones” of soft tissue support.
The soft tissues of the edentulous patient’s jaw are often tender from the effects of thinning mucosa, decreased saliva flow, and unstable and moveable prosthesis. The implant-retained restoration does not require tissue support and improves oral comfort. Finally, speech and function are compromised with removable prostheses, in which the lower complete denture may move as much as 10mm from the supporting structure during function. The tongue and perioral musculature maybe compromised to limit the movement of the mandibular prosthesis. The implant overdenture prosthesis is stable and retentive without the efforts of the musculature and therefore, offer more predictable treatment. Implant supported teeth offer a more predictable treatment course than removable complete dentures. The dental profession, insurance companies, and public are becoming increasingly aware of this.







The aesthetics restoration of facial appearance and improved dental function with implant prosthodontics is directly related to correctly restoring missing intraoral soft and hard tissues and the aesthetics and technical abilities of the dentist and dental technician.l The use of dental implants for oral rehabilitation has revolutionized prosthodontics over the past 3 decades. Multiple studies have proven the efficacy and excellent long-term prognosis with dental implants.2-5
While initial research and clinical use were directed primarily toward the edentulous patient, more recent studies have focused on the aesthetic and functional use of implants in the partially edentulous patient.6 The most challenging area of modern implant dentistry remains the “esthetic zone” in the anterior maxilla and mandible. Replacing multiple anterior teeth in the otherwise dentate patient requires careful consideration of the location and volume of residual bone, soft tissue aesthetics, and room for the implants and prosthesis.
REFERENCES
1. Zarb G, Bolender C, Carlsson, G, Boucher’s Prosthodontic Treatment for Edentulous Patients, Eleventh Edition. St. Louis, The C. V. Mosby Company; 1997.
2. Adell R, Lekholm U, Rockler B, Branemark P-I. A 15-year study of osseointergrated implants in the treatment of edentulous jaw. Int J Oral Surg 1981;10(6):387-416.
3. Branemark P-I., Zarb GA, Alberktsson T (eds). Tissue-Intergrated Prostheses. Osseointergration in Clinical Dentistry. Carol Stream, Il; Quintessence, 1985.Linquist LW,
4. Carlsson GE, Glantz PO. Rehabilation of the edentulous mandible with a tissue- intergrated fixed prothesis: A 6-year longitudinal study. Quintessence Int 1987; 18:89-96
5. Laney WR, Tolman D, Keller EE, Desjard RP, Van Roekel NB, Branemark P-I. Dental implants; Tissue-intergrated prosthesis utilizing the osseointergration concept. Mayo Clin Proc 1986;61(2):91-97.
6. Chiche GJ, Block MS, Pinault A. Implant surgical template for partially edentulous patients. Int J Oral Maxillofac Implants 1989;4:289-292.